Posts
States Re-think Contact Tracing and Case Investigation Strategies as COVID-19 Cases Rise
Contact tracing is an essential strategy for curbing the spread of COVID-19. When implemented quickly, isolation of people diagnosed with COVID-19 and identification and quarantine of close contacts can effectively interrupt disease transmission and reduce spread. Faced with rapidly climbing caseloads, testing delays, and increases in community spread, states and localities have had to prioritize high-risk cases, utilize technology in new ways, and implement creative strategies to conduct case investigations, trace contacts of infected individuals, and perform follow-up.
Contact tracing works best when quick follow-up is possible, sufficient testing resources are available, and when social isolation and quarantine are possible. Due to recent case spikes, contact tracers in some states are unable to call COVID-19-positive individuals fast enough. Additionally, with some regions reaching an accelerating state of community spread, it is more difficult to determine exactly where individuals were exposed to COVID-19. In North Dakota, these issues led to a major shift in contact tracing protocols. Since October, the state has asked infected individuals to notify their close contacts and direct them to resources on the Department of Health’s website.
Recently, other states have followed suit:
- The Maine Center for Disease Control and Prevention will make only one contact with an infected individual (instead of checking in with them periodically) to provide guidance. It will also enroll people in the program based on when their last contact with someone with COVID-19 was. That way, they will enroll people who have the highest number of days left in their 10-day quarantine period so Maine CDC can work with them as early as possible to limit exposure to others in the community. The state is also limiting its contact tracing to high-risk individuals, including those age 65 and older, health care workers, children, individuals of color, school workers, and congregate living facility residents.
- As of mid-November, Nebraska had a backlog of 2,600 people who had tested positive for COVID-19 but had not been contacted by a contact tracer. To address the backlog, the Department of Health and Human Services reduced the number of call attempts from five to two, reduced the number of interview questions, and asked individuals to call their own contacts to let them know they tested positive.
- New Hampshire began focusing on contact tracing for high-risk populations including health care workers, communities of color, and people living in group living spaces. The state is also asking health care providers to educate COVID-19-positive patients about isolation and quarantine procedures.
- Oregon has shifted tracking priorities as its case counts rise drastically to protect the state’s most vulnerable residents in long-term care facilities, jails, foster homes, etc. Contact tracers are still advised to perform the first two steps of tracing: interviewing new COVID-19 cases and finding their contacts and notifying them to get tested and quarantine, but they will no longer do ongoing monitoring of these groups.
- Pennsylvania is prioritizing case investigations of its most vulnerable residents, such as those in nursing homes, or cases that could lead to greater community spread.
- In Wisconsin and Wyoming, only individuals who have tested positive for COVID-19 will hear from contact tracers. Individuals are instructed to reach out to their own close contacts.
Since spring, states have shifted their approaches to contact tracing to reflect current needs. The examples above show that states are currently focused on maximizing contact tracing effectiveness by focusing on known or presumed positive cases and working to protect those at increased risk through a more targeted approach to contact tracing outreach.
Additionally, several of these states have been financing their contact tracing efforts with federal funds and there is some uncertainty about whether these funds will be renewed. With the year drawing to a close, there are competing demands for these resources as states prepare for vaccine distribution and education, and funding has likely played into decisions to cut back instead of hiring new contact tracers.
In response to state actions like the ones above, the US Centers for Disease Control and Prevention (CDC) released new guidance on Dec. 3, 2020, about how to prioritize contact tracing and case investigation in states and jurisdictions where cases are on the rise. The new directions were guided by several principles:
- Maximizing effectiveness;
- Protecting household contacts;
- Preventing outbreaks and clusters; and
- Protecting people at increased risk.
 Source:
Source: Virginia has adopted these guidelines and will join the list of states that are using contact tracing prioritization as a way to address surging cases.
States can use other strategies in their contact tracing work to maximize value, including technology. As of Dec. 1, 17 states were using the Google and Apple exposure notification technology that alerts individuals when they have been in close contact with someone who has tested positive for COVID-19. There is an increasing focus on these phone applications working across state lines as the technology becomes more standardized. In other states, technology is being used to connect people with quarantine resources—a strategy that can make contact tracing more effective.
For example, in Connecticut, a statewide software system called ContaCT monitors test results and positive cases. The ContaCT platform will identify and refer people who need support at initiation and throughout self-isolation or self-quarantine. Case workers will support people in self-isolation or self-quarantine by connecting them with state, local, and regional resources as necessary, such as food and housing.
Other states are using a range of strategies to improve the efficiency or effectiveness of their contact tracing programs in the face of rising caseloads and hospitalization rates:
- The Ohio Department of Health is updating its systems to allow local health departments to enter information about an infected person’s contacts prior to their positive test to get a better idea of where the virus is likely to spread.
- Since August, Washington, DC contact tracing efforts have included home visits for high-risk individuals who did not complete contact tracing interviews or could not be reached by contact tracers.
- North Dakota, South Dakota, and Vermont have recently revived their partnerships with the National Guard to help with elements of contact tracing and case investigation.
- In New Mexico, businesses that have had a confirmed COVID-19 case or exposure among staff can avoid a 14 day Rapid Response Closure by signing a surveillance testing and contact tracing In the document the employers must agree to conduct testing among their staff and select a COVID-19 coordinator responsible for working with the NM Department of Health on contact tracing efforts in the workplace.
- South Dakota is incorporating texting and email into their initial outreach strategy, replacing phone calls in some cases. This approach can be more automated and will allow individuals to input their own information to a secure online portal even if they are unable or unwilling to answer the phone.
Contact tracing is just one piece of the puzzle when it comes to mitigating the spread of COVID-19. Increased public education about the importance of mask wearing and social distancing, as well as increased testing and resources for effective quarantine will also be critical for curbing the spread. As COVID-19 case numbers rise and fluctuate this winter, states are expected to continue to adjust their contact tracing and case investigation strategies to meet their needs and utilize available resources. The National Academy for State Health Policy, in partnership with Mathematica, will continue to track and analyze state efforts.
Support for this work was provided by the Robert Wood Johnson Foundation. The views expressed here do not necessarily reflect the views of the foundation.
How States Are Ramping Up their COVID-19 Contact Tracing Capacity
Contact tracing, a strategy long-used to contain the spread of infectious diseases by identifying and isolating people exposed to an infection, has become a crucial state tool to curb COVID-19. But the pandemic requires significant ramping up of contact tracing capacity and funding. Experts estimate 30 contact tracers are needed for every 100,000 Americans – a total of 98,460 workers nationwide – far short of states’ current tracer workforces.
Confronted with looming budget shortfalls and unknown future federal relief funding, state health departments are taking a variety of approaches to scale up contact tracing. Some are working in-house to increase their state and local workforces, others are partnering with other organizations to secure staffing, training, and recruitment assistance, and others are contracting with a third party.
The National Academy for State Health Policy (NASHP) created an interactive map highlighting how every state and Washington, DC, is innovating and expanding its contact tracing capacity to contain the infection and reopen its economy. Several examples of each model type are described below.
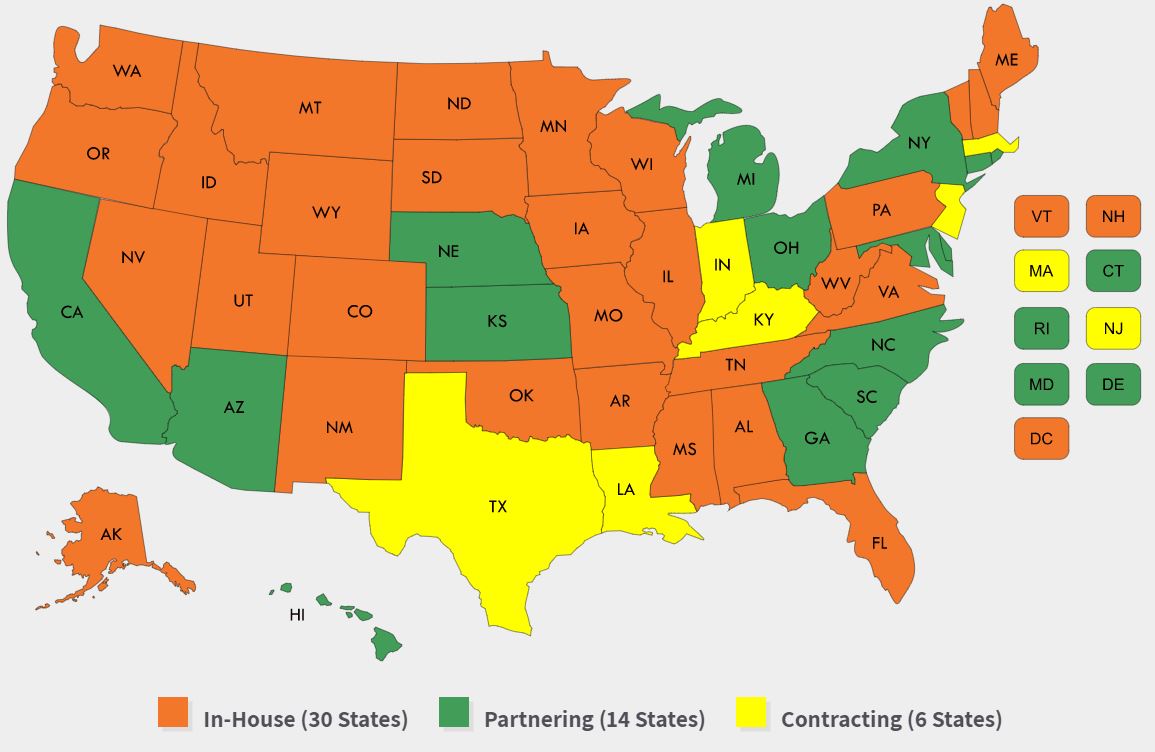 This interactive map highlights each state’s contact tracing program model, workforce, lead agencies, funding, and technology.
This interactive map highlights each state’s contact tracing program model, workforce, lead agencies, funding, and technology.
- In-house: As of late May 2020, more than half of the states are managing contact tracing in-house by increasing their workforces. Many are reassigning internal health department staff along with county and state employees to contact tracing roles, including swimming pool and restaurant inspectors in Nevada and police in Colorado. Washington, DC and several states are hiring contact tracers. DC will use $2.3 million from the city’s contingency ccash reserve fund for its initial hires. Many states are increasing their workforce by seeking volunteers, including Wisconsin, which created a State Emergency Operations Center to organize and train contact tracers and coordinate volunteers from its Emergency Assistance Volunteer Registry. States are also engaging students and partnering with universities, including North Dakota, whose public health graduate students are receiving course credit for their contact tracing work. Several other states, including Delaware, Iowa, Nevada, New Hampshire, Oklahoma, Rhode Island, South Dakota, Washington State, and West Virginia have brought in the National Guard for contact tracing assistance.
- Partnering: Several states have formal partnerships or contracts in place to support their contact tracing efforts. Many states are pursuing this option to train contact tracers. In California, where the state and local health agencies are managing a paid and volunteer workforce, the state awarded an $8.7 million contract to the University of California, San Francisco, to provide training and technical assistance to local health departments. The University of Hawaii Community Colleges are providing training and adding capacity in their community health worker programs so that community health worker graduates will be prepared to support COVID-19 contact tracing in Hawaii. Other states are partnering with third parties to supplement staffing or facilitate recruitment and hiring efforts. In Michigan, the private company Rock Connections will manage volunteers, and Deloitte will manage technology for the state’s tracing program. In North Carolina, the state health department launched the Carolina Community Tracing Collaborative, partnering with two local health care delivery and education organizations, along with Partners in Health, to coordinate with and build on existing contact tracers in local health departments.
- Contracting: Six states have announced plans to contract a large portion of their contact tracing work out to a third party. These states are contracting with private companies or nonprofit organizations, some with call-center settings, to take over or augment a state’s contact tracing workforce. In Indiana, the state awarded a $43 million contract to a private health and human services company, Maximus, to hire about 500 people to staff a call center and manage the state’s ongoing contact tracing effort. State health department officials say this will preserve capacity for state and local health officials to intervene in settings that are at higher risk for outbreaks. Similarly, Texas is contracting with the private technology company, MTX Group, at a cost of nearly $300 million for a 27-month contract to build and manage a group of contact tracers, with a goal of building a workforce of 4,000 tracers. New Jersey announced its Community Contact Tracing Corps will centralize its effort and will be staffed with partnerships with colleges and universities as well as a contract with a vendor. NASHP recently detailed Massachusetts’ Contact Tracing Collaborative, a unique model with the nonprofit Partners in Health, which is managing a virtual support center of up to 1,000 people when fully staffed.
States also vary in their approaches to contact tracing, with some creating a centralized effort led by the state health department and others using an approach led primarily by local health agencies with state support and coordination. In Montana, the state is supporting local efforts through the creation of a grant program using $5 million in federal Coronavirus Aid, Relief and Economic Security (CARES) Act funding, in part, for local health departments, tribal public health, and urban Indian clinics to enhance their COVID-19 contact tracing efforts. New Jersey is shifting to centralize its efforts by building a contact tracing corps that will supplement work that has primarily been led at the local level to date.
In addition to creating a robust contact tracing workforce, states are pursuing a variety of technologic solutions to supplement or facilitate this work. Several states are using automated symptom monitoring systems that allow those who have been in contact with someone with COVID-19 to report symptoms daily. Arizona’s secure, automatic 14-day symptom monitoring and reporting system allows contacts to report symptoms to public health daily by phone, text, or online. Other technological strategies range from statewide platforms that allow the state health department to share data with contact tracers to apps that use Bluetooth location technology to notify users when they have been near someone with COVID-19. The utility of these novel apps remains uncertain due to technical difficulties, public distrust, and potential privacy concerns.
How States Are Funding Contact Tracing
Contact tracing is a costly endeavor, with states reporting spending millions to staff up and create infrastructures either internally or through third parties. The National Association of City and County Health Officials, and other public health associations, have called on the federal government to provide $7.6 billion in emergency supplemental funding to public health agencies to assemble this nationwide team.
In Ohio, the state Controlling Board approved use of federal COVID-19-related funding, including $12.4 million for local health departments for contact tracing in May and June. Virginia committed $58 million in federal emergency aid to expand contact tracing and a pending state bill in Minnesota would direct up to $300 million for contact tracing-related costs, including staffing, a public service campaign, and technology.
While many states report using CARES Act funds (or other federal funds) for their contact tracing efforts, some will also use funds from private donors. Kaiser Permanente Colorado contributed $1 million for suppression of COVID-19 among homeless individuals in Denver and Bloomberg Philanthropies is investing $10.5 million and partnering with Johns Hopkins University for recruitment, training, and deployment of 3,500 contact tracers for New York, New Jersey, and Connecticut. Other private businesses are donating staffing resources – in Massachusetts, Blue Cross Blue Shield provided staff for the state’s contact tracing initiative.
Contact tracing for COVID-19 presents states with an unprecedented challenge that they are meeting by employing unique and creative strategies. With public health funding falling as a proportion of health spending since the early 2000s, chronic under-funding of state and local health agencies has limited states’ ability to quickly scale up to address emergencies. Federal support, collaborative and contractual relationships, and technology solutions are enabling states to take on this evolving need. NASHP will continue to track this dynamic issue and update its State Approaches to Contact Tracing during the COVID-19 Pandemic interactive map over time.
 For individuals living with complex, often chronic conditions, and their families, palliative care can provide relief from symptoms, improve satisfaction and outcomes, and help address critical mental and spiritual needs during difficult times. Now more than ever, there is growing recognition of the importance of palliative care services for individuals with serious illness, such as advance care planning, pain and symptom management, care coordination, and team-based, multi-disciplinary support. These services can help patients and families cope with the symptoms and stressors of disease, better anticipate and avoid crises, and reduce unnecessary and/or unwanted care. While this model is grounded in evidence that demonstrates improved quality of life, better outcomes, and reduced cost for patients, only a fraction of individuals who could benefit from palliative care receive it.
For individuals living with complex, often chronic conditions, and their families, palliative care can provide relief from symptoms, improve satisfaction and outcomes, and help address critical mental and spiritual needs during difficult times. Now more than ever, there is growing recognition of the importance of palliative care services for individuals with serious illness, such as advance care planning, pain and symptom management, care coordination, and team-based, multi-disciplinary support. These services can help patients and families cope with the symptoms and stressors of disease, better anticipate and avoid crises, and reduce unnecessary and/or unwanted care. While this model is grounded in evidence that demonstrates improved quality of life, better outcomes, and reduced cost for patients, only a fraction of individuals who could benefit from palliative care receive it. 























































































































































